






“The single biggest problem in communication is the illusion that it has taken place,” from William Whyte’s 1952 book “Is Anyone Listening?”
Margaret Schwarze, M.D., MPP, FACS used this quote to introduce one of her 3 inspirational and inspiring presentations at the Sommer Memorial Lectures I attended in Portland last week. I have attempted to summarize some of the important material she shared in this column.
“Dr. Schwarze is a board-certified vascular surgeon and medical ethicist. She is a nationally recognized expert in surgical decision-making, informed consent, advance directives, and end-of-life care. Her research focuses on improving communication between older patients and their surgeons so that patients can avoid unwanted treatment and make decisions that align with their values, preferences, and goals.” Our Team | The Patient Preferences Project
Failed communication between doctor and patient is all too common. It can lead to interventions of uncertain necessity, increase costs financially, and cause unnecessary pain and suffering.
It has never been an easy task for a doctor to share bad news and present difficult decisions. Doing so is different in 2024 than it was in the days of Marcus Welby, M.D.
1 - Lack of continuity in modern healthcare. In the past, doctors took care of their patients for years. They chose, knew, and trusted each other. In these times, the doctor more commonly does not know the patient. For surgeons, this change is not as impactful as they have always been called to intervene with a patient they are meeting for the first time and often in a crisis.
2 - Lack of time. Doctors are in short supply, as is the time they are allotted (often by non-clinical managers in healthcare systems) to see patients. Communicating bad news, with the goal of shared decision-making, is not something that can be crammed into a 15-minute visit.
3 - Explosion of technology and possible interventions. In these times, we not only have to share bad news but too many options for what to do about it. When I started training, if you were having a heart attack, we ‘watched you’ in the Cardiac Care Unit using standard medications to avoid fatal complications. Now there are so many options! Cath, stent, bypass, watchful waiting, oh my!
Doctors share ‘the facts.’ The facts, the disease, the pathology in pictures, the percentage risk, the complexity, etc. This is often communicated in medical lingo that is like a foreign language to anyone non-medical.
They/we then assume that the patient understands and that communication has taken place. More commonly than not, the patient does not really ‘get it.’ In a critical situation, patients hear and understand very little. Research has shown that if the word cancer is uttered, the patient hears nothing else. They are too terrified to take any more in! If you need a stent in your heart or your intestine is twisted and only surgery will save your life, that is darn terrifying too.
“Patients don’t need more information, they need more interpretation,” from Ann J Russ and Sharon R. Kaufman in Family Perceptions of Prognosis, Silence and the Suddennes of Death.
This is Dr. Schwartze’s work in a nutshell. Her Mission is:
Better conversations – every surgeon, every patient, every time.
To accomplish this goal, she founded Home | The Patient Preferences Project.
The original research was presented in Engaging Patients, Health Care Professionals, and Community Members to Improve Preoperative Decision Making for Older Adults Facing High-Risk Surgery. JAMA Surg. 2016 Oct 1;151(10):938-945.JAMA Surg. 2016 Oct 1;151(10):938-945.
She feels doctors need to communicate not only details of the pathology (the problem), and the procedure (the surgical intervention) but what really can be expected from the intervention. It is important to dispel myths about what surgery can and cannot accomplish.
When the patient asks, “What would you do if I were your father?” Dr. Schwartze feels we have an obligation to answer the question. To decline is a cop-out.
However, to answer that question, we need to know our patients. What do they enjoy and live for? What are their values? What is important to them? How are they thinking about this?
Expectations need to be explained for every step of the way: post-operative (what to expect when I wake up), the recovery process, and long-term results. Thorough and realistic for every step.
She shared a story at the lectures (to a group of 300 mixed physicians) of a colleague’s elderly patient who underwent an aortic repair after a typical ‘communication’ (or the illusion thereof). The patient and family were told the usual percentages and they thought it was the ‘best case scenario.’ There is only a 50% risk of dying from surgery and gave the green light. After a successful surgery, the family found Mom in the ICU with tubes coming out of every orifice and were horrified, totally unprepared for this expected post-operative support. “Our Mom would have never wanted this! Please stop now and take all of those tubes out!”
Uncertainty always hovers in a medical exam room and is part and parcel of the practice of medicine. This is perhaps something non-medical people don’t understand or want to believe. It takes a confident and honest physician to communicate uncertainty in a way that is understood by the patient and their family.
To do so she has found surprising challenges in study design. Nonetheless, she persists.
Her team is working on a study in End Stage Renal Disease of patients with or without concurrent palliative care when the time comes to consider beginning dialysis. Palliative care physicians and nurses are the experts in communicating bad news and consideration of the steps in decision-making. Does their involvement with the patients improve communication and outcomes in a difficult chronic disease situation? Outcomes include peace of mind and comfort as well as longevity.
While the research studies slowly rolled out, Dr. Schwartze and her team created a TEACHING tool to help doctors communicate with patients. She calls it Best Case/Worst Case Scenario and has taught thousands of doctors to use this tool through lectures, cartoons (yes!), and videos. You can see those on the website above though it is a tool for doctors.
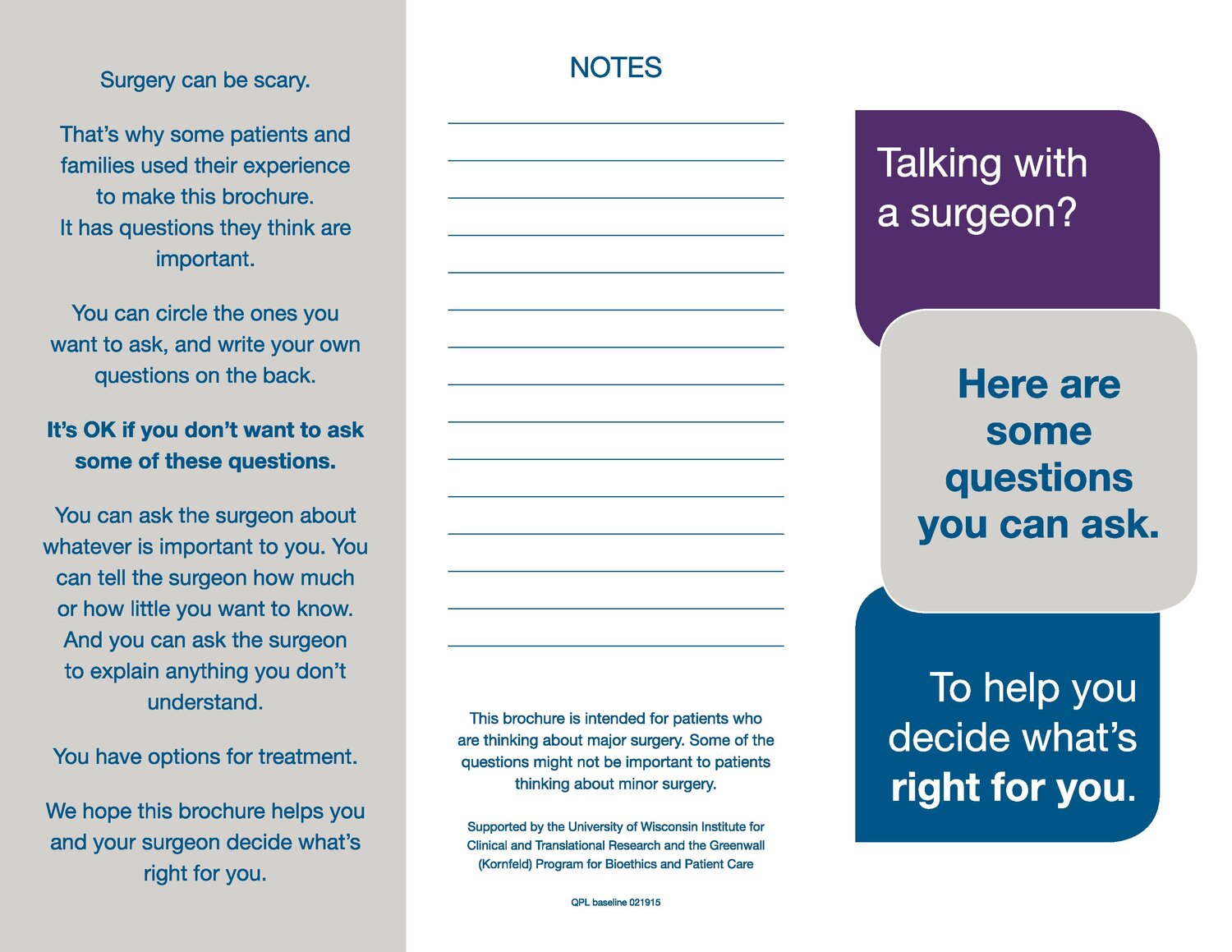
In addition, the team has developed a Question Prompt List for YOU, the patient facing a serious medical decision.
Question Prompt List | The Patient Preferences Project
The prompt list is a series of questions designed to help older adults make a decision about high-risk surgery. These same questions are relevant to any major intervention being proposed such as dialysis and cancer treatment. I encourage you to download the above brochure for a time in the future when you need to be prepared for an important doctor's appointment.
Here is the Question Prompt List:
I - Should I have surgery?
- What are my options?
- What is likely to happen if I have surgery? If I don’t have surgery?
- In your opinion, will surgery make me feel better?
- In your opinion, will surgery help me live longer? If so, how much longer?
II - What should I expect if everything goes well?
- How do you think my daily life will look after surgery? Right after, in 3 months and one year later?
- Will I have tubes and drains put in during or after surgery? Will I need them at home?
- In your opinion, how will this surgery affect my other health problems (such as diabetes or high blood pressure)?
- After I leave the hospital, what type of care do you think I will need?
III - What happens if things go wrong after surgery?
- Can you describe serious complications and explain what those might mean to me?
- If I’m too sick to speak for myself, how can I make sure you know my wishes?
- If I decide to appoint someone to make medical decisions for me, what do I need to do to make those arrangements official?
Know Thyself, inscribed upon the Temple of Apollo in the ancient Greek precinct of Delphi. Know what you love about life, what matters to you, and your values for living. Consider all of this for yourself, and share it with your doctor, as you face a serious medical decision.
While Dr. Schwartze and her team are educating physicians about how to talk to you, you can use these questions and tools to advocate for yourself and your loved ones.
Debra L. Glasser, M.D., is a retired internal medicine physician in Olympia. Got a question for her? Write drdebra@theJOLTnews.com





2 comments on this item Please log in to comment by clicking here

KarenLJ
My mother was an RN, and shared hospital stories with us kids. From an early age, we were familiar with medical terminology. As we all got older, we considered ourselves lucky that in the face of new medical issues, we at least didn't have to learn a new language. I hope that most doctors can take the time to define terms for their patients and families, so they're not overwhelmed by words they don't understand. They have enough to deal with.
Wednesday, May 8 Report this
mtndancer
Thank you for this list of questions! It is also helpful to have a recorder (either recording device or friend taking notes) with you in the consultation room. You cannot process all the information the doctor must give you in the limited time they are allotted to give it. Any medical provider should allow a recording device!
Wednesday, May 8 Report this